

Dietary Protein Q&A
Dietary Protein Q&A
Answers to your common questions as well as some insight into other aspects and myths.

As someone involved in the health & fitness landscape from a personal enthusiast, an aspiring professional in the world of dietetics and in the sports world of strength & human performance, I often get questions from the likes of clients, family members and friends concerning topics that circle around about everything you can think of. I find FAQ’s pretty useful in a lot of scenarios because more than likely, someone else has the exact same question you do. This series is going to cover protein-related questions solely. I’m currently building out more nutritional concerns as well as exercise and performance questions which will be released once it’s a little more refined. Any questions that went unanswered or want a more in-depth reply, feel free to drop me a comment or get in touch.
These recommendations are purely based on current scientific evidence and any chronic conditions where nutrition heavily comes into play should be discussed further by your PCP or specialist you see. With that being said…
Your total daily energy expenditure (how much energy/calories you’re burning) is what’s coming into play regarding how much of any macronutrient is advisable and what type of dietary preferences you follow. This needs to be taken into account with every single category and topic that’s covered. These amounts though, can be broken up depending on food preference, lifestyle and exercise habits. If a person consumes more energy (calories) than what they expend, weight gain will occur. It’s simply the law of thermodynamics.
Dietary Protein: FAQ’s & Answers
How Much Protein Should I Eat?
Consuming enough protein is crucial, especially for anyone following a weight-management plan, whether they're trying to gain, lose, or maintain weight. When someone starts to lose weight, body fat and lean body mass (LBM) are typically both lost simultaneously (32). Increasing your protein intake is essential to preventing this. Sustainability on any calorie deficit is affected by the loss of LBM since it lowers metabolic rate and overall energy expenditure. In addition to fatigue, deterioration in neuromuscular performance, and an elevated risk of injury (29). A subsequent body fat overshoot, or a rebound in fat mass, is caused by the metabolic decline that follows LBM loss (7), which leads to negative, compounded changes in body composition. The current RDA for dietary protein sits at 0.8g/kg/day (28) but more studies coming out are really pushing for that number to be much higher. Additionally, it is recommended that protein should make up between 10% and 35% of daily calories. It appears that around 1.4–2.0g/kg/day is the recommended amount that should really be suggested (15). I think that the average person should strive to at least reach that floor of 1.4g/kg/day whereas athletes and highly active individuals should aim for the higher end. Body weight is often expressed in science by kilograms (kg). For anyone in america and the western world using pounds (lb) simply divide your body weight by 2.2 and you should get your weight in kg. For example: a 150lb woman (68.2kg) and 95-136g of protein recommended. In comparison, a 200lb man (90.1kg) and 127-180g of protein recommended.
Any reason to worry about protein distribution throughout the day?
This systematic review by Hudson & colleagues (16) compared more frequent, moderate-sized protein servings with fewer, larger servings that are distributed more evenly throughout the day. The researchers showed that both protein distribution patterns produced comparable gains in lean body mass, which is in contrast to the hypothesis that more frequent, moderate-sized protein doses should be preferable to less frequent, bigger protein servings. However, ingesting protein with meals as opposed to in between them led to a more steady loss of fat mass. I feel like the literature is pretty firm in terms of making sure to get your optimal daily protein intake in with each corresponding meal. This is probably due to 1.) ensuring enough daily protein is met to keep in a positive nitrogen balance and 2.) to optimally stimulate muscle protein synthesis with each serving of protein
How important is protein when reducing caloric intake or dieting?
As previously discussed, protein intake is essential to maintaining lean body mass, which will maintain your resting metabolic rate, especially while you are on any kind of calorie-restricted diet. It has been demonstrated that the intake, as well as increasing it above average, is very advantageous to health in general and during a weight-management strategy (6,14). The feeling of fullness, or satiety, is another important factor to take into account while reducing your daily caloric intake. When protein is consumed, a variety of hormones are released that may cause you to feel full (31). Examining the amount of your daily protein consumption is a good thing to do when dieting and experiencing increased feelings of hunger.
Are men and women the same in terms of protein needs?
Luckily, we have a randomized control trial showing this exactly (20). It’s been found that protein needs really don’t differ too much between the sexes, and the sliding recommendations still apply based on body weight. Again, more active females should look to be closer to the top.

Can I drink a protein shake to make up the difference at the end of the day?
I like this question because it gives me a chance to talk about our elderly, aging population, a group that is both under-served and discussed. Skeletal muscle weakens and loses mass as a person gets older often leading to a diagnosis of sarcopenia. According to estimates, sarcopenia has developed from this muscle fragility in 10% of those over the age of 60 (11). To answer the question, yes. You can definitely include a protein shake or smoothie in your everyday diet. Whey protein will also be your greatest option for optimum protein digestion if your stomach can handle it. Whey is a high-quality, quickly absorbed dairy protein that is frequently used in the general population, and according to a recent review by Gilmartin and colleagues (11), consuming 35g of whey daily as a dietary supplement will likely enhance sarcopenic biomarkers in those with that condition. Having trouble getting enough protein in for the day? A protein shake is a great option.
Any truth in a high protein diet being bad for your kidneys?
It can be tough to really parse this question out to deliver an appropriate answer because it’s actually a very layered topic and condition regarding the kidneys. Even when researching this question, the research surrounding a diet high in protein has a wealth of information sitting on different sides of the aisle regarding its safety.
We’re asking about kidney health here in regards to protein intake. Because of that, let's look into chronic kidney disease (CKD). CKD is a disease that has multifactorial pathophysiology associated with it, meaning it has quite a few underlying factors that could begin its initiation. I’m going to discuss two lab values; estimated glomerular filtration rate (eGFR) and Uric Acid (UA). eGFR relates to how well your kidneys are working overall and UA is a byproduct of purines being produced in the body from different substances you ingest, both food and beverage.
It’s possible it’s the way different study designs are put into place that cause us to sometimes get mixed results, not really allowing for a definitive answer. A lot of very recent work has come out about this exact topic which was nice to see. A 2022 study (27) on the aging population in Japan looked into comparing the amount of dietary protein intake on any changes in renal function, specifically eGFR. The results concluded that these individuals on average were consuming protein around 1.5g/kg/day and proved to be beneficial in at least maintaining their current eGFR value.
Before we dive deeper, it's important to note that the current 2020 CKD guidelines recommend anywhere between .55 - .8g/kg/day in those with and without diabetes signaling a low protein diet (17). Looking into more information seemingly skewing in both directions, includes work from the American Diabetes Association (23) suggesting no harm at all to a diet higher in protein. The ranges for that study were around .9 - 1.6g/kg so certainly higher than before but still not huge by any means. Another factor to bring in entirely was proposed from a study by Narasaki & colleagues (22). They brought up an interesting point related to “where” and the “source” of the protein being extremely important, which leads us to discuss Uric Acid.
There is a lot of talk about the breakdown of dietary proteins and raising systemic UA levels, but a 2018 meta-analysis (19) discovered seven types of food (beer, wine, liquor, soft drinks, poultry, potatoes) and three types of meat (beef, pork, and lamb) that were linked to high serum UA levels as well as eight other foods with lower serum UA levels but higher protein levels (eggs, skim milk, brown bread, non-citrus fruits, cheese, cereals, etc.)
When UA is present inside of cells, it displays a pro-oxidant behavior that increases the production of free radicals and pro-inflammatory cytokines, decreases the bioavailability of vasodilator substances (widening of blood vessels) and increases the bioavailability of vasoconstrictor (narrowing) substances like angiotensin, all of which contribute to oxidative stress (13), chronic inflammation, and endothelial dysfunction, the three factors that contribute to the initiation and progression of CKD (18). UA levels are a reliable indicator of the onset and progression of CKD. According to several reports, the prevalence of hyperuricemia gradually rises as renal function declines, becoming 10x more common in CKD stages 3-5 than in stage 1. (26). This connection draws attention to a possible advantage of detecting UA through screening at various stages of CKD (1). Recent research confirms the link between high UA levels and the initiation and accelerated development of several chronic illnesses, including CKD, cardiovascular risk (10), metabolic syndrome, and cognitive decline (8).
Let’s delve into this “sourcing” a little bit here by discussing plant-based diets (PBD) and protein related to CKD. PBDs have been used successfully in interventional studies to prevent and treat serious coronary heart disease (3), type 2 diabetes, early-stage low-grade prostate cancer (24), and obesity (30). A PBD pattern is consistently linked to a low incidence and mortality of cancer and cardiovascular disorders in studies of centenarians (those who live to be 100 years old or older) from various geographical areas (4). These populations limit their fish and meat intake and typically eat diets that are rich in complex and low in refined carbohydrates. Studies comparing UA serum concentrations in vegetarians and non-vegetarians have consistently revealed a lower average UA serum concentration in vegetarians, which is relevant to the relationship between the cumulative effect of plant-based nutrition and serum UA level. Studies have shown that high total protein intake is not related with higher blood urate (UA) and that consumption of plant-based protein may be negatively associated with hyperuricemia and gout (commonly tied to uric acid levels as well), despite the fact that purine-restricted diets are frequently lower in protein (5).
Where does this leave us? Consume less protein, eat a low protein diet in fear of having an increased risk of higher uric acid levels? I don’t really think the data shows that that’s correct. As we’ve seen, other foods and beverages can contribute to this. Although some meat products certainly show this, it’s also intake of refined carbohydrates and sugar sweetened beverages that increase the risk as well. Sounds like poor diet quality might be the big factor here.
I’m Vegetarian/Vegan, is protein from plants providing the same benefit?
If you’re looking for a response from me bashing or throwing dirt on a vegetarian or vegan diet… you’re really out of luck. The benefits of switching to, or even altering your current nutrition towards even a “little more” plant-based than you might be can have some very pronounced effects toward your overall health, as we just witnessed through discussing these changes in light of UA levels and CKD.
Regarding the specific intake of protein here. The dynamics between daily rates of muscle protein synthesis (MPS) and breakdown (MPB) controls how much muscle you maintain (21). The fact that plant-based proteins lack the complete amino acid profile that most animal sources do is what causes this matter to be so hotly contested. Leucine, an amino acid, has been strongly linked to promoting muscle protein synthesis when ingested both at rest and during the post-exercise window (2). Enough necessary amino acids are needed as precursors to enable effective muscle protein accretion, in addition to triggering the signaling pathways that increases muscle protein synthesis. Due to the fact that it lacks the whole spectrum of amino acids, plant protein is frequently criticized in this area (9). It's vital to note that, in contrast to the anabolic response of animal-based proteins, not ALL plant proteins are digested in the same way. There are many different plant-based proteins available (12). In a recent study, these plant-based proteins were compared across the board (25).
Besides having a relatively low essential amino acid content (i.e. low leucine content), many plant-based proteins are deficient in one or more specific amino acids. Plant-based proteins are often particularly low in lysine and/or methionine content. The easiest way to compensate for the lower protein quality of a plant-based versus animal-based protein source is to simply consume a greater amount, and from different sources.
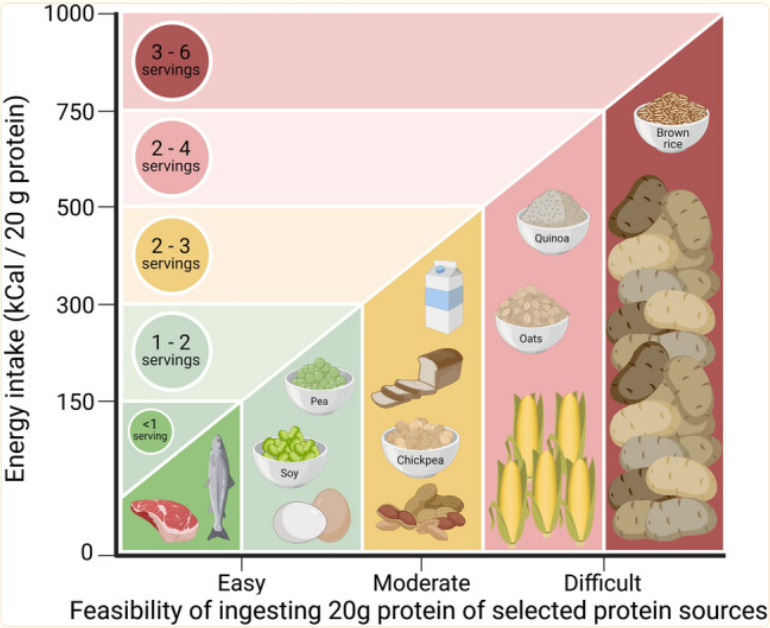
Here’s an example that was put forth (12); because corn, hemp, brown rice, soy, and pea protein are low in lysine and/or methionine, for instance, this shortage could be made up for by ingesting 2-4 times more of the same protein from each source. However, adding equal amounts of soy or pea protein plus corn, hemp, or brown rice protein—all of which have low lysine and high methionine content—provides a blend with a more balanced amino acid profile. Such mixtures would only need 1.1–1.9 times more protein to make up for particular amino acid deficits.